 Fiberglass Hazard Research
Fiberglass Hazard Research
Hazards of large fibers vs
Hazards & detection of very small fiberglass fragments

- POST a QUESTION or COMMENT about fiberglass dust, particle, & mold hazards in buildings
Research studies on fiberglass hazards in buildings supporting our article series about how to identify fiberglass insulation in buildings and fiberglass hazards and fiberglass insulation contamination issues in residential and light-commercial buildings.
InspectAPedia tolerates no conflicts of interest. We have no relationship with advertisers, products, or services discussed at this website.
- Daniel Friedman, Publisher/Editor/Author - See WHO ARE WE?
Fiberglass & Mineral or Synthetic Fiber Exposure Hazard Research, Standards & Regulations
 The fiberglass research literature is replete with studies indicating that there are no health hazards associated with airborne fiberglass particles, and with other studies reaching quite the opposite conclusion, some citing Fiberglass Lung Disease (Hsu 2024).
The fiberglass research literature is replete with studies indicating that there are no health hazards associated with airborne fiberglass particles, and with other studies reaching quite the opposite conclusion, some citing Fiberglass Lung Disease (Hsu 2024).
First listed in the Seventh Annual Report on Carcinogens (1994) as Glass Wool (Respirable Size), In 2021 an NIH study concluded that certain glass wool fibers (inhalable) can be reasonably anticipated to be a human carcinogen. (NIH 2021).
Reviewing the literature we find some studies asserting that it's the very small particles that are more-hazardous (Ilinois DOH 2018) while others point to longer fibers as more-hazardous (Madl 2022).
Our OPINION is that because of the technical difficulty of detecting very small fiberglass particles their presence and healh impact could have been under-stated.
Our OPINION is that prudent avoidance of inhaling fiberglass dust and using damp wiping and HEPA vaccuming to clean up significant levels of such dust in occupied spaces would be in order. - Daniel Friedman 2025
Watch out: We recommend that readers examine carefully the methodology used in these studies, the expertise of the researchers, and the sources financing of such work (for potential conflicting interests).
- Abbate, Carmelo, Concetto Giorgianni, Renato Brecciaroli, Giovanni Giacobbe, Chiara Costa, Vittorio Cavallari, Francesca Albiero et al. "CHANGES INDUCED BY EXPOSURE OF THE HUMAN LUNG TO GLASS FIBER–REINFORCED PLASTIC." [PDF] Environmental health perspectives 114, no. 11 (2006): 1725-1729.
Abstract
The inhalation of glass dusts mixed in resin, generally known as glass fiber–reinforced plastic (GRP), represents a little-studied occupational hazard.
The few studies performed have highlighted nonspecific lung disorders in animals and in humans.
In the present study we evaluated the alteration of the respiratory system and the pathogenic mechanisms causing the changes in a group of working men employed in different GRP processing operations and exposed to production dusts.
The study was conducted on a sample of 29 male subjects whose mean age was 37 years and mean length of service 11 years.
All of the subjects were submitted to a clinical check-up, basic tests, and bronchoalveolar lavage (BAL); microscopic studies and biochemical analysis were performed on the BAL fluid.
Tests of respiratory function showed a large number of obstructive syndromes; scanning electron microscopy highlighted qualitative and quantitative alterations of the alveolar macrophages; and transmission electron microscopy revealed the presence of electron-dense cytoplasmatic inclusions indicating intense and active phlogosis (external inflammation).
Biochemical analyses highlighted an increase in protein content associated with alterations of the lung oxidant/antioxidant homeostasis.
Inhalation of GRP, independent of environmental concentration, causes alterations of the cellular and humoral components of pulmonary interstitium; these alterations are identified microscopically as acute alveolitis. - Abtahi, Shabnam, Mahyar Malekzadeh, Ghafour Nikravan, and Abbas Ghaderi. "Measurement of lung cancer tumor markers in a glass wool company workers exposed to respirable synthetic vitreous fiber and dust." The international journal of occupational and environmental medicine 9, no. 1 (2018): 23.
Abstract Excerpts:
Results: Individuals exposed to higher than the recommended levels of respirable SVF had higher serum concentrations of CEA and CYFRA 21-1, compared to controls (p=0.008 and 0.040, respectively), as well as in comparison to those exposed to lower than recommended OSHA levels (p=0.046 and 0.033, respectively).
Workers with >9 years work experience, had significantly (p=0.045) higher levels of serum CYFRA 21-1 than those with ≤9 years of experience.
Conclusion: It seems that working for >9 years in sites with detectable levels of respirable SVF and dust would increase the levels of known lung cancer serum tumor markers.
Transferring these workers to sites with respirable SVF concentrations lower than the limit of detection in the air is recommended. - [2] Accurate Plastics Inc., ACCULAM™ MEGAGLAS [PDF] trade name "NEMA Grades G5/G9", Accurate Plastics, Inc. 18 Morris Place Yonkers, NY 10705-1929, Tel: 914-476-0700, Composition: Fiberglass & Melamine/formaldehyde Resin, retrieved 10/21/2012, original source: http://www.acculam.com/MSDS-Melaglas.pdf
- Albrecht, Matthew A., Cameron W. Evans, and Colin L. Raston. "Green chemistry and the health implications of nanoparticles." Green chemistry 8, no. 5 (2006): 417-432.
- ATSDR Synthetic Vitreous Fibers, Public Health Statement [PDF] U.S. CDC, retrieved 2025/-4/22 local copy on file as Synthetic-Vitreous-Fibers-ATSDR.pdf
Excerpts:
Results from animal experiments show that when synthetic vitreous fibers or other inhaled dust particles are deposited in the deepest part of the lung in high numbers, the lung responds with a process called pulmonary inflammation. In this process, macrophage numbers in the lung increase so that they can engulf and move the fibers out of the lung.
When high numbers of fibers are deposited, the macrophages can become clumped together.
If pulmonary inflammation continues, the cells lining the lung may thicken from a process called bronchiolization. Bronchiolization may reduce the amount of oxygen that the body gets from the air during breathing.
If exposure stops, deposited synthetic vitreous fibers slowly dissolve in the lung fluid or are moved out of the lung by the macrophages, and pulmonary inflammation disappears with time.
Results from animal studies also show that repeatedly breathing high levels of some types of synthetic vitreous fibers may cause a slow buildup of scar-like tissue in the lungs and in the membrane surrounding the lungs.
This scar-like tissue does not expand and contract like normal lung tissue, and breathing can become difficult.
- Babin, Angela. Health hazards manual for artists. Rowman & Littlefield, 2008.
- Baier, R., A. Meyer, D. Glaves-Rapp, E. Axelson, R. Forsberg, M. Kozak, and P. Nickerson. "The body's response to inadvertent implants: Respirable particles in lung tissues." The Journal of Adhesion 74, no. 1-4 (2000): 103-124.
Abstract
Instillation of respirable glass fibers to rat lungs served as an in vivo model for the detection and evaluation of differential local biological responses to particulate matter in the deep lung.
Three compositions of vitreous glass, stonewool, and refractory fiber materials (MMVF 10, HT, and RCF1a) were harvested with surrounding lung tissues and examined both histologically and by physical/chemical assays to correlate the observed differential dissolution events with specific biological responses associated with each material.
Specimens at 2-days, 7-days, 30-days and 90-days post-instillation were compared from at least three rats for each condition and for phosphate-buffered-saline controls. HT fiber surface and bulk chemistry uniquely allowed direct histochemical visualization of fiber degradation steps by Prussian Blue staining, while multiple attenuated internal reflection infrared spectroscopy and energy-dispersive X-ray analysis of unfixed, fresh lung lobe slice surfaces revealed the concurrent biochemical changes.
Insulation glass (MMVF 10) dissolved most quickly in extracellular compartments, as well as after phagocytosis of small fragments; stonewool (HT) was externally thinned by surrounding phagocytes and fragmented into shorter lengths engulfable by macrophages;
refractory ceramic (RCF1a) resisted both external dissolution and macrophage uptake, becoming embedded in granulomatous nodules.
It is clear from these results that the lung can process inadvertently respired particulates in different ways dependent on the specific compositions of the particles.
The animal model and analytical scheme reported here also show substantial promise for evaluating the effects of bioaerosols, and synergistic effects of respirable toxins with particulates, and consequences of dental aspirates into the lung. - Berrigan, David. "Respiratory cancer and exposure to man‐made vitreous fibers: A systematic review." American journal of industrial medicine 42, no. 4 (2002): 354-362.
Abstract Excerpt:
The results highlight the difficulty of assessing small increases in risk of respiratory cancer potentially caused by occupational exposure in populations with high prevalence of tobacco use. - Boffetta, Paolo, Ken Donaldson, Suresh Moolgavkar, and Jack S. Mandel. "A systematic review of occupational exposure to synthetic vitreous fibers and mesothelioma." Critical reviews in toxicology 44, no. 5 (2014): 436-449.
Abstract:
Objective
We investigated whether available epidemiological and toxicological data suggest an increased risk of mesothelioma among workers exposed to synthetic vitreous fibers (SVF). Methods We conducted a systematic review of epidemiological studies on the risk of mesothelioma among workers exposed to SVF, and toxicological studies on SVF and mesothelioma.
Results
Seven cohort studies were conducted among workers employed in production of rock/slag wool, glass wool, or continuous glass filament in the United States, Canada, and Europe. Of the six deaths from mesothelioma identified in these studies, three had exposure to asbestos. A review of death certificates in a study of rock wool production workers identified one additional probable death.
A formal comparison with expected deaths is not feasible. Four community-based case–control studies were identified, of which three reported an increased risk among SVF-exposed workers. The number of cases not exposed to asbestos was less, and residual confounding from asbestos exposure misclassification may explain the association in these studies.
The toxicology review of SVF suggested that they present a low hazard mostly due to their low biopersistence, typically with a half-life in rat studies of tens of days compared to amphibole asbestos which has a half-life of 400–500 days.
Conclusions
The combined evidence from epidemiology and toxicology provide little evidence that exposure to SVF increases the risk of mesothelioma. - Breum, N. O., Thomas Schneider, O. Jørgensen, T. Valdbjørn Rasmussen, and S. Skibstrup Eriksen. "CELLULOSIC BUILDING INSULATION VERSUS MINERAL WOOL, FIBERGLASS OR PERLITE: INSTALLER’S EXPOSURE BY INHALATION OF FIBERS, DUST, ENDOTOXIN AND FIRE-RETARDANT ADDITIVES." [PDF] Annals of occupational hygiene 47, no. 8 (2003): 653-669.
Abstract: A task-specific exposure matrix was designed for workers installing building insulation materials. A priori, a matrix element was defined by type of task (installer or helper), type of work area (attic spaces or wall cavities) and type of insulation material (slabs from mineral wool, fiberglass or flax; loose-fill cellulosic material or perlite).
In the laboratory a mock-up (full scale) of a one-family house was used for simulated installation of insulation materials (four replicates per matrix element). Personal exposure to dust and fibers was measured.
The dust was analyzed for content of endotoxin and some trace elements (boron and aluminum) from fire-retardant or mold-resistant additives. Fibers were characterized as WHO fibers or non-WHO fibers. In support of the exposure matrix, the dustiness of all the materials was measured in a rotating drum tester.
For installers in attic spaces, risk of exposure was low for inhalation of dust and WHO fibers from slab materials of mineral wool or fiberglass. Slab materials from flax may cause high risk of exposure to endotoxin.
The risk of exposure by inhalation of dust from loose-fill materials was high for installers in attic spaces and for some of the materials risk of exposure was high for boron and aluminum. Exposure by inhalation of cellulosic WHO fibers was high but little is known about the health effects and a risk assessment is not possible.
For the insulation of walls, the risk of installers’ exposure by inhalation of dust and fibers was low for the slab materials, while a high risk was observed for loose-fill materials. The exposure to WHO fibers was positively correlated to the dust exposure.
A dust level of 6.1 mg/m3 was shown to be useful as a proxy for screening exposure to WHO fibers in excess of 106 fibers/m3. In the rotating drum, slabs of insulation material from mineral wool or fiberglass were tested as not dusty. Cellulosic loose-fill materials were tested as very dusty, and perlite proved to be extremely dusty.
Concusions:
For installers in attic spaces, risk of exposure was low by inhalation of dust and WHO fibers from slab materials of mineral wool or fiberglass. Slab materials from flax may cause high risk of exposure to endotoxin. The risk of exposure to dust from loosefill materials was high for installers in attic spaces and for some of the materials risk of exposure was high for elements (boron and aluminum) from fire- or mold-resistant additives.
Exposure to cellulosic WHO fibers was high, but little is known about the health effects and a risk assessment is not possible.
For the insulation of walls, the risk of installers’ exposure to dust and fibers was low for the slab materials, while a high risk was observed for loose-fill materials. Exposure to WHO fibers was positively correlated to the dust exposure.
A dust level of 6.1 mg/m3 was shown to be useful as proxy for screening exposure to WHO fibers in excess of 106 fibers/m3. Slabs of insulation material from mineral wool or fiberglass were tested not dusty, while cellulosic loose-fill materials were tested very dusty and perlite proved extremely dusty. - Bounoughaz, Moussa, and Noura Touabi. "The self ignition of fiberglass lines." International Letters of Chemistry, Physics and Astronomy 20 (2014).
- Brandt-Rauf, P. W., L. F. Fallon, T. Tarantini, Cathy Idema, and L. Andrews. "Health hazards of fire fighters: exposure assessment." Occupational and Environmental Medicine 45, no. 9 (1988): 606-612.
- Castillo, Jeffrey E. "Fiberglass-Information You Should Know." Professional Safety 37, no. 11 (1992): 29.
- Davis, John MG. "A review of experimental evidence for the carcinogenicity of man-made vitreous fibers." Scandinavian journal of work, environment & health (1986): 12-17.
- Dear, Joseh A., OSHA PEL for FIBERGLASS, INTERPRETATION (letter) [PDF], OSHA, retrieved: 02/26/2023 original source: https://www.osha.gov/laws-regs/standardinterpretations/1995-10-06-3#:~:text=The - 8 hour TWA PEL level of exposure, risk of adverse health effects.
- El Safty, A., S. Helal, N. Abdel Maksoud, and A. Samir. "Occupational Health Hazards among Double Sided Printed Circuit Board Manufacturers." British Journal of Applied Science & Technology 4, no. 11 (2014): 1634.
Note: cites fiberglass-induced dermatitis. - [7] Energy Saving Trust, www.energysavingtrust.org.uk/Energy-saving-assumptions [this link will open in a new window] , (03/13). Actual savings depend on individual circumstances. Contact: 020 7654-2455, email foundation@est.org.uk

- Fiberglass carcinogenicity: "GLASS WOOL FIBERS EXPERT PANEL REPORT, PART B - RECOMMENDATION FOR LISTING STATUS FOR GLASS WOOL FIBERS AND SCIENTIFIC JUSTIFICATION FOR THE RECOMMENDATION",
The Report on Carcinogens (RoC) expert panel for glass wool fibers exposures met at the Sheraton Chapel Hill Hotel, Chapel Hill, North Carolina on June 9-10, 2009, to peer review the draft background document on glass wool fibers exposures and make a recommendation for listing status in the 12th Edition of the RoC.
The National Institute of Environmental Health Sciences is one of the National Institutes of Health within the U.S. Department of Health and Human Services.
The National Toxicology Program is headquartered on the NIEHS campus in Research Triangle Park, NC.
Following a discussion of the body of knowledge, the expert panel reviewed the RoC listing criteria and made its recommendation.
The expert panel recommended by a vote of 8 yes/0 no that glass wool fibers, with the exception of special fibers of concern (characterized physically below), should not be classified either as known to be a human carcinogen or reasonably anticipated to be a human carcinogen.
The expert panel also recommended by a vote of 7 yes/0 no/1 abstention, based on sufficient evidence of carcinogenicity in well-conducted animal inhalation studies, that special-purpose glass fibers with the physical characteristics as follows longer, thinner, less soluble fibers (for 1 example, > 15 μm length with a kdis of < 100 ng/cm2/h) are reasonably anticipated to be a human carcinogen for the listing status in the RoC.
The major considerations discussed that led the panel to its recommendation include the observations of tumors in multiple species of animals (rats and hamsters).
Both inhalation and intraperitoneal routes of exposure produced tumors, although inhalation was considered more relevant for humans. - [4] FIBERGLASS INSULATION MOLD: occurrence of mold contamination in fiberglass insulation can be impossible to see with the naked eye, but can be significant
- Fisher, A. A. "Fiberglass vs mineral wool (rockwool) dermatitis." Cutis 29, no. 5 (1982): 412-415.
Abstract:
Fiberglass and rockwool dermatitis is usually due to a mechanical irritant reaction. When several members of a family are affected, scabies is often initially suspected.
The irritant dermatitis may be complicated by an urticarial and an eczematous reaction which may mimic an allergic reaction clinically and histologically.
Allergic reactions to added epoxy or formaldehyde resins may very rarely occur. - Galimany, Eve, Montserrat Ramón, and Maximino Delgado. "First evidence of fiberglass ingestion by a marine invertebrate (Mytilus galloprovincialis L.) in a NW Mediterranean estuary." Marine pollution bulletin 58, no. 9 (2009): 1334-1338
- Gualtieri, A. F. "Mineral fibre-based building materials and their health hazards." In Toxicity of Building Materials, pp. 166-195. 2012.
Focused on asbestos hazards. - Gwaltney-Brant, Sharon M., Lisa A. Murphy, Tina A. Wismer, and Jay C. Albretsen. GENERAL TOXICOLOGIC HAZARDS AND RISKS FOR SEARCH-AND-RESCUE DOGS RESPONDING TO URBAN DISASTERS [PDF] Journal of the American Veterinary Medical Association 222, no. 3 (2003): 292-295.
Note: this studyh points out on p. 7 that workers exposed to styrene in the production of fiberglass-reinforced plastic sheets sufrfered genotoxic effects. " They found that the exposed workers showed significantly high levels of DNA strand breaks (p < 0.0001) and a drastic decrease in DNA repair activity as compared with the controls ... " - Op. Cit. p. 7 - Helal, Sawsan Farouk, and Wessam Sabry Elshafy. HEALTH HAZARDS AMONG WORKERS IN PLASTIC INDUSTRYy [PDF] Toxicology and industrial health 29, no. 9 (2013): 812-819.
- Hsieh, Meng Ying, Yueliang Leon Guo, Judith Shu Chu Shiao, and Hamm Ming Sheu. "Morphology of glass fibers in electronics workers with fiberglass dermatitis–a scanning electron microscopy study." International journal of dermatology 40, no. 4 (2001): 258-261.
- Hogan, Daniel J., and Megan Morrison. "Fiberglass, Dusts." In Kanerva's Occupational Dermatology, pp. 415-426. Springer, Berlin, Heidelberg, 2012.
Abstract
Production of fiberglass is increasing. Airborne dermatitis may be caused by fiberglass.
Irritant contact dermatitis is usually caused by fibers greater in diameter.
Hardening is not prominent and may be less likely development atopics Histopathology of dermatitis is nonspecific unless the fiberglass is itself visualized in the skin biopsy or skin tape stripping.
Treatment is nonspecific except for taking measures to curtail exposure to fiberglass and where possible to identify sources of exposure. - Hossain, Niamat Ullah Ibne, Farjana Nur, and Raed M. Jaradat. "An analytical study of hazards and risks in the shipbuilding industry." In Proceedings of American Society for Engineering Management Annual Conference, pp. 18-21. 2016.
Excerpt:
Most of these production areas, which include welding, painting, blasting, and fiberglass production have a direct effect on workers' health … - Hsu, Chan-Yang, Hsin-Yi Chen, Min-Shiau Hsieh, Yi-Hsin Lee, Chou-Chin Lan, and Mei-Chen Yang. CONSTRICTIVE PERICARDITIS IN A PATIENT WITH FIBERGLASS LUNG DISEASE: A CASE REPORT [PDF] BMC Pulmonary Medicine 24, no. 1 (2024): 382. - 2025/04/22 original source: https://link.springer.com/article/10.1186/s12890-024-03192-6
Abstract Excerpts:
Background
Fiberglass has a larger aerodynamic diameter and is less likely to be inhaled into the lungs.
Further, it will be cleared even if it is mechanically broken into smaller pieces and inhaled into the lungs.
Fiberglass lung disease has been well documented if long term exposure but was thought reversible and would not cause severe diseases.
The diagnosis of fiberglass lung disease depends on exposure history and histopathological findings.
However, the exact occupational exposure history is often difficult to identify because mixed substance exposure often occurs and fiberglass disease is not as well-known as asbestosis. ...
Conclusion
Fiberglass could cause inflammation of the pericardium, resulting in pericardial effusion and constrictive pericarditis, which could be severe and require radical pericardiectomy. Exact exposure history and histopathological examinations are the key to diagnosis.
Keywords Asbestosis body, Constrictive pericarditis, Fiberglass lung disease, Pericardial effusion, Radical pericardiectomy - IARC Working Group on the Evaluation of Carcinogenic Risks to Humans, International Agency for Research on Cancer, and World Health Organization. Man-made vitreous fibres. No. 81. World Health Organization, 2002.
- IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Man-made Vitreous Fibres. Lyon (FR): International Agency for Research on Cancer; 2002. (IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, No. 81.) GENERAL REMARKS ON MAN-MADE VITREOUS FIBRES [Web article] Available from: https://www.ncbi.nlm.nih.gov/books/NBK396448/ - retrieved 2025/04/22
Excerpts:
This eighty-first volume of IARC Monographs considers certain man-made vitreous (glass-like) fibres of highly variable composition that are widely used for thermal and acoustical insulation and to a lesser extent for other purposes. The generic term, man-made vitreous fibres (MMVFs), denotes non-crystalline, fibrous inorganic substances (silicates) made primarily from rock, slag, glass or other processed minerals.
These fibres, also called man-made mineral fibres, include glass fibres (used in glass wool and continuous glass filament), rock (stone)/slag wool and refractory ceramic fibres.
Rock (stone) wool, slag wool and glass wool are used extensively in thermal and acoustical insulation, typically in buildings, vehicles and appliances.
The refractory ceramic fibres are designed for high-temperature applications, mainly in industrial settings. Continuous glass filament is used primarily in reinforced composite materials for the insulation, electronics and construction industries.
These substances were evaluated by a previous IARC Working Group (IARC, 1988) (Table 1). Since these evaluations, new data have become available, which have been incorporated into the monograph and were taken into consideration in the present evaluations.
...
Man-made vitreous fibres have some physical similarities to asbestos, in particular, their fibrous character which gives them the same aerodynamic properties and leads to their deposition throughout the respiratory tract.
Unlike amphibole asbestos, however, they are synthetic and amorphous, and generally have a lower biopersistence in lung tissues.
Also, unlike serpentine asbestos, they tend to break transversely rather than cleaving along the fibre axis. [
This is perfectly consistent with our own forensic lab work (see FIBERGLASS IDENTIFICATION in the LAB as shown in our photo below, of the concoidal fracture at the end of a fiberglass fragment, consistent with training in forensic microscopy and the identifiation of fiberglass fibres at McCrone Research - Ed.]

Inhaled asbestos fibres can cause two quite different malignancies in humans: malignant mesothelioma, which arises from the lining of the body cavities, and carcinoma of the lung, which arises from pulmonary epithelial cells (IARC, 1987).
Epidemiological studies of human populations exposed to MMVFs have therefore focused on these two types of cancer.The mechanisms of carcinogenesis by inhaled fibres and the use of data on these mechanisms in the identification of carcinogenic hazard have been reviewed by Kane et al. (1996).
- [6] IARC MONOGRAPHS ON THE IDENTIFICATION OF CARCINOGENIC HAZARDS TO HUMANS [Website] (2025) Original website: https://monographs.iarc.fr/ (large PDF over 6MB)
https://publications.iarc.fr/ENG/Monographs/vol81/mono81-6A.pdf - article details - [2025/04/22 dead link - Ed.]
https://publications.iarc.fr/ENG/Monographs/vol81/mono81-6C.pdf - studies of cancer in experimental animals in re vitreous fibers such as fiberglass;
https://publications.iarc.fr/ENG/Monographs/vol81/mono81-6E.pdf - summary of data reported & evaluation
https://publications.iarc.fr/ENG/Monographs/vol81/mono81-6F.pdf for the article references
To search the IARC monographs on various environmental concerns and carcinogens, use https://publications.iarc.fr/ENG/Monographs/PDFs/index.php


- Illinois DOH, FIBERGLASS - ENVIRONMENTAL FACT SHEET [PDF], (2018) Illinois Department of Public Health
Division of Environmental Health
525 W. Jefferson St.
Springfield , IL 62761 USA, TEl: 217-782-5830 retrieved 2018/07/11, original source: http://www.idph.state.il.us/envhealth/factsheets/fiberglass.htm
Excerpt:
Little information is known about the health effects caused by small fibers.
Smaller fibers have the ability to reach the lower part of the lungs increasing the chance of adverse health effects.
People who work with fiberglass or who have worn-out duct work lined with fiberglass in their homes or workplace may have long-term exposure to fiberglass.
There is no evidence that fiberglass causes cancer in people. Animal studies have shown an increased risk of cancer when fiberglass fibers were implanted in the lung tissue of rats, but these studies are controversial because of how the fibers were implanted.
Based on these animal studies, the International Agency for Research on Cancer has classified some fibers used in fiberglass as possible human carcinogens (cancer causing agents). - Infante, Peter F., Loretta D. Schuman, and James Huff. "Fibrous glass insulation and cancer: response and rebuttal." American journal of industrial medicine 30, no. 1 (1996): 113-120.
- Kim, Seong Chan, Matthew S. Harrington, and David YH Pui. "Experimental study of nanoparticles penetration through commercial filter media." In Nanotechnology and Occupational Health, pp. 117-125. Springer, Dordrecht, 2006.
- Lent, Tom, FORMALDEHYDE EMISSIONS FROM FIBERGLASS INSULATION WITH PHENOL FORMALDEHYDE BINDER [PDF] (2009) Healthy Building Network 2446 West St Berkeley, CA 94702 tlent@healthybuilding.net www.healthybuilding.net
- Lim, Hyun Sul, Yun Chul Hong, Jung Ran Kim, Hae Kwan Cheong, Ji Yong Kim, Nam Won Paik, Hoe Kyeong Cheong, and Chong Han Lem. "An epidemiologic study on the health hazards of inhabitants chronically exposed to glass fiber." Korean Journal of Epidemiology 17, no. 1 (1995): 76-93.
- Lipworth, Loren, Carlo La Vecchia, Cristina Bosetti, and Joseph K. McLaughlin. "Occupational exposure to rock wool and glass wool and risk of cancers of the lung and the head and neck: a systematic review and meta-analysis." Journal of occupational and environmental medicine 51, no. 9 (2009): 1075-1087.
Excerpt: Conclusions: Despite a small elevation in RR for lung cancer among MMVF production workers, the lack of excess risk among end users, the absence of any dose-risk relation, the likelihood of detection bias, and the potential for residual confounding by smoking and asbestos exposure argue against a carcinogenic effect of MMVF, RW, or GW at this time.
Similar conclusions apply to HN cancer risk among workers exposed to MMVF.
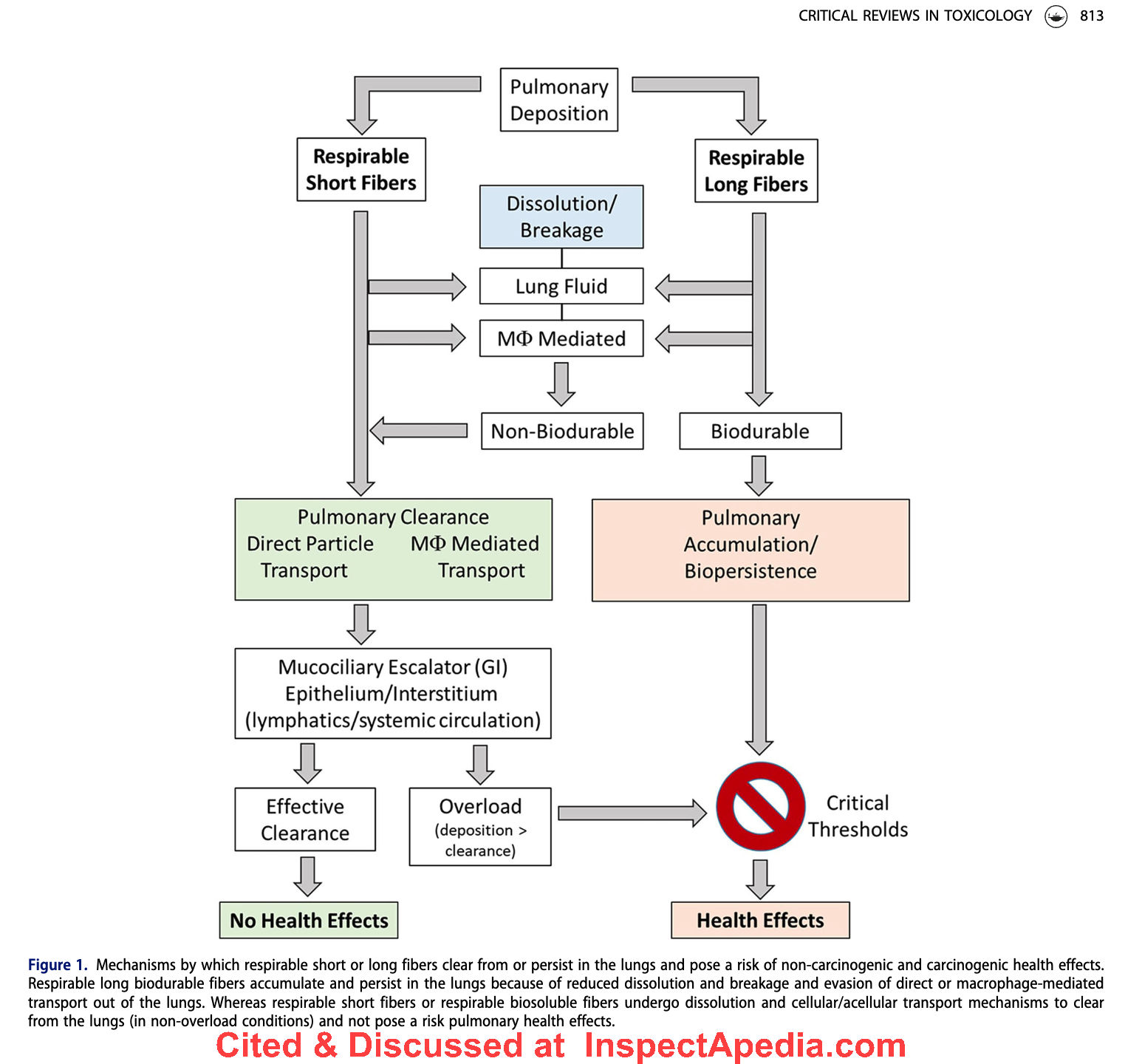
Above: pathway of possible health effects of deposits of fiberglass fragments in the lung (Madl 2022).
- Madl, A. K., & O’Neill, H. C. (2022). Fiber biodurability and biopersistence: historical toxicological perspective of synthetic vitreous fibers (SVFs), the long fiber paradigm, and implications for advanced materials. Critical Reviews in Toxicology, 52(10), 811–866. https://doi.org/10.1080/10408444.2022.2154636 - local copy saved as Fiber-biodurability-SVFs-Madl.pdf
Abstract excerpts:
Extensive toxicology studies of synthetic vitreous fibers (SVFs) demonstrated that fiber dimension, dur-ability/dissolution, and biopersistence are critical factors for risk of fibrogenesis and carcinogenesis.Lessons learned from the SVF experience provide useful context for predicting hazards and risk of nano-enabled advanced materials.
This review provides (1) a historical toxicological overview of animal andin vitro toxicology studies of SVFs,
(2) key findings that long durable fibers pose a risk of fibrogenic andtumorigenic responses and not short fibers or long soluble fibers,
(3) in vitro and in vivo test methods forbiodurability and biopersistence and associated predictive thresholds for fibrosis or tumors, and
(4) recommendations for testing of advanced materials.
Generally, SVFs (fiber lengths >20 mm) with in vitro fiberdissolution rates greater than 100 ng/cm2/hr (glass fibers in pH 7 and stone fibers in pH 4.5) and in vivofiber clearance less than WT1/2 40 or 50 days were not associated with fibrosis or tumors.
Long biodura-ble and biopersistent fibers exceeding these fiber dissolution and clearance thresholds may pose a risk offibrosis and cancer.
Fiber length-, durability-, and biopersistent-dependent factors that influence patho-genicity of mineral fibers are also expected to affect the biological effects of high aspect ratio nanomate-rials (HARN).
Only with studies aimed to correlate in vitro durability, in vivo biopersistence, and biologicaloutcomes will it be determined whether similar or different in vitro fiber dissolution and in vivo half-lifethresholds, which exempt carcinogenicity classification of SVFs, can also apply to HARNs.
- Marsh, Gary M., Ada O. Youk, Roslyn A. Stone, Jeanine M. Buchanich, Mary Jean Gula, Thomas J. Smith, and Margaret M. Quinn. "Historical cohort study of US man-made vitreous fiber production workers: I. 1992 fiberglass cohort follow-up: initial findings." Journal of occupational and environmental medicine 43, no. 9 (2001): 741-756.
Abstract:
This 1986 to 1992 update and expansion of an earlier historical cohort study examined the 1946 to 1992 mortality experience of 32,110 workers employed for 1 year or more during 1945 to 1978 at any of 10 US fiberglass (FG) manufacturing plants. Included are
(1) a new historical exposure reconstruction for respirable glass fibers and several co-exposures (arsenic, asbestos, asphalt, epoxy, formaldehyde, polycyclic aromatic hydrocarbons, phenolics, silica, styrene, and urea); and
(2) a nested, matched case-control study of 631 respiratory system cancer (RSC) deaths in male workers during 1970 to 1992 with interview data on tobacco smoking history.
Our findings to date from external comparisons based on standardized mortality ratios (SMRs) in the cohort study provide no evidence of excess mortality risk from all causes combined, all cancers combined, and non-malignant respiratory disease.
Also, excluding RSC, we observed no evidence of excess mortality risk from any of the other cause-of-death categories considered. For RSC among the total cohort, we observed a 6% excess (P = 0.05) based on 874 deaths. Among long-term workers (5 or more years of employment) we observed a not statistically significant 3% excess based on 496 deaths.
Among the total cohort, we observed increases in RSC SMRs with calendar time and time since first employment, but these were less pronounced among long-term workers.
RSC SMRs were not related to duration of employment among the total cohort or long-term workers. In an externally controlled analysis of male workers at risk between 1970 and 1992, we observed no association between RSC SMRs and increasing exposure to respirable FG.
Our findings to date from internal comparisons based on rate ratios in the case-control study of RSC were limited to analyses of categorized study variables with and without adjustment for smoking.
On the basis of these analyses, the duration of exposure and cumulative exposure to respirable FG at the levels encountered at the study plants did not appear to be associated with an increased risk of RSC. RSC risk also did not seem to increase with time since first employment.
There is some evidence of elevated RSC risk associated with non-baseline levels of average intensity of exposure to respirable glass, but when adjusted for smoking this was not statistically significant, and there was no apparent trend with increasing exposure.
This same pattern of findings was observed for duration of exposure, cumulative exposure, and average intensity of exposure to formaldehyde.
None of the other individual co-exposures encountered in the study plants appeared to be associated with an increased risk of RSC.
The primary focus of ongoing analyses is to determine the extent to which our present findings are robust to alternative characterizations of exposure.

- Marsh, Gary M., Autumn Bernal, Natalie Suder Egnot, Marisa Kreider, Shabnam Abtahi, Mahyar Malekzadeh, Ghafour Nikravan, and Abbas Ghaderi. COMMENTS ON THE MEASUREMENT OF LUNG CANCER TUMOR MARKERS IN WORKERS OF A GLASS WOOL COMPANY [PDF] Int J Occup Environ Med (The IJOEM) 9, no. 3 July (2018): 1356-157.
Dear Editor,
We read with interest the article on the measurement of lung cancer tumor markers in a group of workers exposed to respirable synthetic vitreous fiber (SVF) and dust, recently published in the IJOEM.1
The authors report on the relationship between exposure to respirable SVF and serum levels of two biomarkers implicated in lung cancer, suggesting that elevations in these biomarkers support a relationship between SVF exposure and lung cancer.
However, several methodological and interpretational issues in their evaluation call the authors' conclusions into question.
For example, the authors excluded smokers only from the study's control group, thus any effects of smoking would differentially influence any statistical comparisons made between the cases and controls.
Moreover, the authors' basic two-sample statistical comparisons did not enable adjustment for the potential confounding factors including known risk factors for cancer such as age, alcohol use, and family history. In the Introduction of their paper, the authors also grossly misinterpreted the overwhelmingly negative scientific literature as providing evidence of a positive association between exposure to SVF and several lung diseases including lung cancer and pleural mesothelioma.
In addition to methodological flaws, the authors misrepresented the meaningfulness of the reported elevations in biomarker levels.
The authors suggest that these biomarkers, carcinoembryonic antigen (CEA) and cytokeratin 19 fragment (CYFRA 21-1), are useful diagnostic and prognostic tools for lung cancer.
Based on the literature cited, it is clear that neither CEA nor CYFRA 21-1 consistently displays diagnostic value.2,3 Furthermore, these biomarkers are not specific to lung cancer. Nearly all of the observed associations reported in this study1 attenuate after excluding smokers from the analysis and are no longer statistically significant.
The main conclusion of the Abtahi, et al, study that remained statistically significant following the exclusion of smokers, is based on findings from a stratified analysis comparing workers by duration of employment (greater vs less than nine years).
Age is a known prognostic factor for lung cancer and a possible source of heterogeneity in biomarker levels.4,5
Therefore, the reported higher levels of CYFRA 21-1 among workers employed by the glass fiber manufacturing facility for greater than nine years may simply be due to the older ages among those with longer durations of employment. Lastly, for CEA and CYFRA 21-1 to have a prognostic value, both require concentrations in the blood higher than those reported in this cohort.
Therefore, Abtahi, et al, relied on premises not supported by the scientific literature, that these biomarkers, at concentrations similar to those present in this cohort, have both diagnostic and prognostic values for prediction of lung cancer.
In conclusion, the recommendations set forth by Abtahi, et al, are not evidence-based.
Neither the methodology nor the interpretation provided supports the authors' conclusions that their study suggests an increased risk of lung cancer in SVF-exposed workers.
Therefore, their recommendation to move workers to areas with non-detectable concentrations of SVF is unwarranted based on their work.
Conflicts of Interest and Financial Disclosure: The North American Insulation and Manufacturer's Association has sponsored a research contract with Cardno ChemRisk.
The funding association had no involvement or influence in the analysis, writing or conclusions of this Letter.
Dr. Marsh is also a Professor of Biostatistics, Epidemiology and Clinical and Translational Science, and Director, Center for Occupational Biostatistics and Epidemiology, University of Pittsburgh, Graduate School of Public Health.
References
Abtahi S, Malekzadeh M, Nikravan G, Ghaderi A. Measurement of lung cancer tumor markers in a glass wool company workers exposed to respirable synthetic vitreous fiber and dust. Int J Occup Environ Med 2018;9:23-31.
Chu XY, Hou XB, Song WA, et al. Diagnostic values of SCC, CEA, Cyfra21-1 and NSE for lung cancer in patients with suspicious pulmonary masses: a single center analysis. Cancer Biology & Therapy 2011;11:995-1000.
Grunnet M, Sorensen JB. Carcinoembryonic antigen (CEA) as tumor marker in lung cancer. Lung Cancer 2012;76:138-43.
Buccheri G, Torchio P, Ferrigno D. Clinical equivalence of two cytokeratin markers in mon-small cell lung cancer: a study of tissue polypeptide antigen and cytokeratin 19 fragments.
Chest 2003;124:622-32. Xu Y, Xu L, Qiu M, et al. Prognostic value of serum cytokeratin 19 fragments (Cyfra 21-1) in patients with non-small cell lung cancer. Scientific Reports 2015;5:9444. Authors' Reply
Dear Editor,
We would like to thank Marsh, et al, for their comments. In our study, we observed that long-term exposure to respirable SVF and dust is associated with higher serum levels of CYFRA 21-1, an indicator of any lung injury including [but not specific to] lung cancer.
Smokers were excluded from the control group; however, 13 out of 145 individuals in the case group were smoker. To eliminate this confounding variable, we excluded the smokers from our cases and re-ran the statistical analyses.
However, the results had been much more reliable if we would have matched our cases and controls for smoking.
The cases and controls we selected were age- and sex-matched. None of the cases and controls was alcohol users.
Nor did they have history of lung cancer in their family members. In the Introduction section of our article, we clearly state that SVF is classified as a group 3 agent (not carcinogen to humans) by IARC.
1 Some sub-groups of SVF (including refractory ceramic fibers) are, however, considered carcinogen.
2 Nonetheless, there is inadequate evidence for human carcinogenicity of other subtypes.
Our study was cross-sectional and mostly observational rather than analytical. We have reported what was observed. The definite worthiness of the serum markers will be determined in long-term follow-up of participants
. Regarding the cited articles and the values of CEA and CYFRA 21-1, the articles mostly discuss the prognostic value of these markers (as mentioned in our article), not their diagnostic value.
As we have mentioned in our article, elevation of these markers has been observed in several disease conditions including chronic airway inflammatory diseases, chest trauma, and acute respiratory disease syndrome (ARDS);3,4 they are not specific for lung cancer. In our study, we observed that smoking has a considerable association with serum CYFRA 21-1 level.
After excluding smokers, the obtained p value still remained near significant (p=0.056). We believe that larger sample sizes could help to gain more powerful insights into these findings.
Regarding the comment on the age difference between workers with work experience greater vs less than nine years, we agree with Marsh, et al; the two groups were not age-matched (p=0.03).
We would like to point out once again that our study was a cross-sectional (not a cohort) study and that there is no sure way to draw any cause-and-effect relationship solely based on our observations.
There could be other possible explanations for our observations; these serum markers, referred to as lung cancer markers, may elevate in many conditions.
Shabnam Abtahi, Mahyar Malekzadeh, Ghafour Nikravan, Abbas Ghaderi - McCurdy, Stephen A. "Carcinogenicity of Synthetic Mineral Fibers." Western Journal of Medicine 148, no. 1 (1988): 75. retrieved 2018/07/11, original source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1026018/pdf/westjmed00137-0077b.pdf
Text:
Carcinogenicity of Synthetic Mineral Fibers
SYNTHETIC MINERAL FIBERS such as fiberglass and mineral wools have assumed significant industrial importance and currently represent a $3 billion domestic industry.
The durability, strength, and insulating properties of these fibers allow them to serve a wide variety of purposes, including insulation and structural support.
Recognized health risks associated with synthetic mineral fibers include respiratory and skin irritation. They have been considered safe from the standpoint of cancer risk, making their use attractive in applications previously limited to asbestos fibers.
Recent epidemiologic data suggest, however, that synthetic mineral fibers may be associated with increased lung cancer risk.
Concern over possible carcinogenic effects was raised in the early 1970s when it was shown that mesotheliomas could be caused in animals by instilling vitreous fibers into the pleural space.
Fibers that were long, thin, and durable showed a carcinogenic potential equivalent to asbestos. Inhalation studies in animals, however, which probably represent a more appropriate model of human exposure, did not show these fibers to be carcinogenic or significantly fibrogenic.
Epidemiologic studies in human populations have also raised important questions regarding the health risks associated with synthetic mineral fibers.
An increased prevalence of minimal interstitial changes has been found in chest radiographs of insulation plant workers exposed to these fibers.
A large cooperative European study of more than 20,000 workers employed in the industry since the late 1930s showed an excess of lung cancers.
Subjects whose first exposure occurred more than 20 years before the diagnosis of cancer and who began work in the early technologic phase of the industry's development were most strongly affected and had about a twofold increased lung cancer mortality.
Similar results were reported among American workers in the industry.
In comparison, lung cancer deaths among asbestos workers are increased fivefold in nonsmokers and 50-fold in smokers. Insufficient data are available to address the role of smoking for patients with lung cancer associated with synthetic mineral fiber exposure.
Malignant mesothelioma has not been linked to such exposure.
Excess lung cancers in these studies appear concentrated in groups that began working in the industry before protective measures, such as dust suppression, were widely introduced, which probably have significantly reduced exposure for contemporary workers.
If the potential of these fibers to cause lung cancer is dose-related, as is the case for asbestos, then it is likely that less risk accrues to today's workers and that the danger to homeowners with attic insulation of synthetic mineral fiber is negligible.
Measures to minimize exposure should be consistently and conscientiously applied, however, to avoid the tragic health and economic consequences associated with occupational exposures to asbestos.
- STEPHEN A. McCURDY, MD, MPH Sacramento, California
REFERENCES
Enterline PE, Marsh GM: The health of workers in the MMMF industry-Biological effects of man-made mineral fibers, In Guthe T (Ed): Proceedings of a WHO/IARC Conference in Association With JEMRB and TIMA, Copenhagen, 1982, Vol 1. Copenhagen, World Health Organization, Regional Office for Europe, 1984, pp 31 1-339
Simonato L, Fletcher AC, Cherrie J, et al: The man-made mineral fiber European historical cohort study: Extension of the follow-up. Scand J Work Environ Health 1986; 12 (suppl):34-47
Weill H, Hughes J, Hammad YY, et al: Respiratory health of workers exposed to MMMF-Biological effects of man-made mineral fibers, In Guthe T (Ed): Proceedings of a WHO/IARC Conference in Association With JEMRB and TIMA, Copenhagen, 1982, Vol 1. Copenhagen, World Health Organization, Regional Office for Europe, 1984, pp387-412 - NIH, National Librarhy of Medicine, National Center for Biotehnology Information, National Toxicology Program. 15th Report on Carcinogens [Internet]. Research Triangle Park (NC): National Toxicology Program; 2021 Dec 21. Certain Glass Wool Fibers (Inhalable) [Website with full article text] CAS No.: none assigned. Available from: https://www.ncbi.nlm.nih.gov/books/NBK590892/ - retrieved 2025/04/22
Excerpts:
Reasonably anticipated to be a human carcinogen
First listed in the Seventh Annual Report on Carcinogens (1994) as Glass Wool (Respirable Size)
Cancer Studies in Humans
The data available from studies in humans are inadequate to evaluate the relationship between human cancer and exposure to glass wool fibers. Although studies of occupational exposure found excess lung-cancer mortality or incidence, it is unclear that the excess lung cancer was due to exposure specifically to glass wool fibers, because
(1) no clear positive exposure-response relationships were observed (however, misclassification of exposure is a concern), and
(2) the magnitudes of the risk estimates were small enough to potentially be explained by co-exposure to tobacco smoking. [Note: at other points in the article authors also point to a co-exposure to asbestos - Ed.]Mesothelioma
The available data are inadequate to evaluate the association between glass wool exposure and mesothelioma, a rare cancer strongly linked to asbestos exposure.
Mesothelioma was evaluated in detail only for the U.S. cohort; in the other studies, the reporting on mesothelioma either was not specific for exposure to glass wool fibers (Engholm et al. 1987, Rödelsperger et al. 2001) or did not evaluate co-exposure to asbestos (Boffetta et al. 1997).
In the U.S. cohort, two cases of mesothelioma were identified among workers with exposure to glass wool but without known exposure to asbestos; in one case, there was uncertainty in the cancer diagnosis, and in the other case, information on asbestos exposure was not complete (Marsh et al. 2001a). - Neghab, M., and A. Alipour. "Respiratory Health Following Long Term Occupational Exposure to Fiberglass Dust." Iranian Red Crescent Medical Journal 12, no. 2 (2010): 145.
Abstract excerpt:
Conclusion: The results support that exposure to fiberglass dust is unlikely to be associated with respiratory symptoms, abnormal radiographic changes or functional impairments of the lungs. - New Jersey DEHSS, FIBROUS GLASS, HAZRDOUS SUBSTANCE FACT SHEET [PDF], New Jersey Department of Health and Senior Services, retrieved 2018/07/11, original source: https://nj.gov/health/eoh/rtkweb/documents/fs/0933.pdf
- NAIMA, North American Insulation Manufacturers Association, 11 Canal Center Plaza Suite 103, Alexandria VA 22314 USA, Tel: 703-684-0084 Website: https://insulationinstitute.org
Website excerpts:
NAIMA (North American Insulation Manufacturers Association) is the recognized voice of the insulation industry, bringing together North American manufacturers of fiberglass and mineral wool insulation products. - Original source: https://insulationinstitute.org/about-naima/
NAIMA and its members are committed to protecting the health and safety of consumers, employees and workers who manufacture and install fiberglass, rock wool, and slag wool insulation products. NAIMA cooperates with government organizations to provide documentation that demonstrates that the products are safe to manufacture, install and use.
NAIMA and its members have invested tens of millions of dollars in independent health and safety research projects in the United States and abroad.
Fiberglass, rock wool and slag wool insulation products are supported by over 75 years of scientific research.
This research, aimed at investigating the possible human health effects of insulation products, includes epidemiological studies, worker health studies, research with laboratory animals, exposure studies, and fiber biosolubility studies. - Original source: https://insulationinstitute.org/about-naima/health-and-safety/
References: [this is the only citation on this page]: 1. This is a mechanical irritation, not a chemical irritation, and does not meet the US OSHA HAZCOM definition of “irritation” specified in Appendix A to 29 C.F.R. 1910.1200. - Nogueira, Ana, Paulo Morais, Ana Paula Cunha, and Filomena Azevedo. "Systemic allergic contact dermatitis to fiberglass in a factory worker of wind turbine blades." Cutaneous and ocular toxicology 30, no. 3 (2011): 228-230.
- Oldenburg, Marcus, Ute Latza, and Xaver Baur. "Exposure–response relationship between endotoxin exposure and lung function impairment in cotton textile workers." International archives of occupational and environmental health 80, no. 5 (2007): 388-395.
- Robertson, Gray. "Source, Nature, and Symptomology of Indoor Air Pollutants." In Indoor Air Quality, pp. 393-402. Springer, Berlin, Heidelberg, 1990.
Excerpt:... with fiberglass and dermatitis-type reactions are not infrequent due to airborne fiberglass particles... - Rom, William N., and Arthur M. Langer. "Carcinogenicity of Fibrous Glass." Western Journal of Medicine 126, no. 5 (1977): 413.
- Sertoli, A., S. Francalanci, and S. Giorgini. "Fiberglass dermatitis." In Handbook of Occupational Dermatology, pp. 122-134. Springer, Berlin, Heidelberg, 2000.
- Stanton, Mearl F., Maxwell Layard, Andrew Tegeris, Eliza Miller, Margaret May, and Elizabeth Kent. "Carcinogenicity of fibrous glass: pleural response in the rat in relation to fiber dimension." Journal of the National Cancer Institute 58, no. 3 (1977): 587-603.
Abstract:
Seventeen fibrous glasses of diverse type or dimensional distribution induced different incidences of malignant mesenchymal neoplasms when implanted in the pleurae of female Osborne-Mendel rats for periods of more than 1 year.
Neoplastic response correlated well with the dimensional distribution of fibers.
Fibers less than or equal to 1.5 µ in diameter and greater than 8 µ in length yielded the highest probability of pleural sarcomas, and probability trends suggested that pleural sarcoma incidence increased with increasing lengths of fibers with diameters of less than 1.5 µ.
Morphologic observations indicated that fibers less than or equal to 8 µ in length were inactivated by phagocytosis. In fibers greater than 8 µ in length, the correlation of carcinogenicity with increasing length was difficult to explain.
Since neoplastic response to a variety of types of durable fibers, particularly asbestos fibers, was similar, our experiments reinforce the idea that the carcinogenicity of fibers depends on dimension and durability rather than physicochemical properties and emphasize that all respirable fibers be viewed with caution. - Synthetic Mineral Fibers (OSHA web page). This page provides links to OSHA standards, health effects, exposure evaluation, possible solutions and other information - see http://www.osha.gov/SLTC/syntheticmineralfibers/ We excerpt from this page just above.
- Syracuse Research Corporation. Toxicological Profile for Synthetic Vitreous Fibers. US Department of Health and Human Services, Public Health Service, Agency for Toxic Substances and Disease Registry, 2004.
- Takahashi, Toru, Mitsuru Munakata, Hiroyuki Takekawa, Yukihiko Homma, and Yoshikazu Kawakami. "Pulmonary fibrosis in a carpenter with long‐lasting exposure to fiberglass." American journal of industrial medicine 30, no. 5 (1996): 596-600.
- 1910 Subpart Z, Toxic and hazardous substances [related topic page]
- 1910.1000, Air contaminants
Table Z-3, [ https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=9994 ] Mineral dusts.Contains permissible exposure limits (PELs) for "Inert or Nuisance Dust" (respirable fraction and total dust); these are currently the only PELs applicable to synthetic mineral fibers for General Industry.
- 1910.1000, Air contaminants
- OSHA "FIBERGLASS AND THE HAZARD COMMUNICATION STANDARD" [PDF] (1991) by OSHA - retrieved 2016/02/16 from www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=INTERPRETATIONS&p_id=20459
This is an interpretation letter, not a standard, but it offers helpful explanations. - Hill, J. W., W. S. Whitehead, J. D. Cameron, and G. A. Hedgecock. "Glass fibres: absence of pulmonary hazard in production workers." Occupational and Environmental Medicine 30, no. 2 (1973): 174-179.
- Koh, D., I. S. Foulds, and T. C. Aw. "Dermatological hazards in the electronics industry." Contact Dermatitis 22, no. 1 (1990): 1-7.
- Mauderly, Joe L. "Relevance of particle-induced rat lung tumors for assessing lung carcinogenic hazard and human lung cancer risk." Environmental Health Perspectives 105, no. Suppl 5 (1997): 1337.
Abstract excerpt:
Rats and other rodents are exposed by inhalation to identify agents that might present hazards for lung cancer in humans exposed by inhalation.
In some cases, the results are used in attempts to develop quantitative estimates of human lung cancer risk. This report reviews evidence for the usefulness of the rat for evaluation of lung cancer hazards from inhaled particles. - Milne, James. "Are glass fibres carcinogenic to man? A critical appraisal." British journal of industrial medicine 33, no. 1 (1976): 47.
- [1] Panolam, FIBERGLASS REINFORCED PLASTIC (FRP) [PDF] Panolam Industries International Inc. 325 DeSoto Avenue Morristown, TN 37816 (423) 587-1842, retrieved 10/21/2012, original source: http://www.panolam.com/frp/FRP/PDF/FRP_msds_9.28.09.pdf
- Quinn, Margaret M., Thomas J. Smith, Ada O. Youk, Gary M. Marsh, Roslyn A. Stone, Jeanine M. Buchanich, and Mary Jean Gula. "Historical cohort study of US man-made vitreous fiber production workers: VIII. Exposure-specific job analysis." Journal of occupational and environmental medicine 43, no. 9 (2001): 824-834.
Abstract:
All jobs held by a cohort of US man-made vitreous fiber production workers were analyzed for airborne fiber exposure.
This exposure-specific job analysis was part of an exposure assessment for an epidemiologic study of mortality patterns, with particular focus on respiratory cancer, among 35,145 workers employed in 10 fiberglass and five rock or slag wool plants.
The exposure assessment was conducted from the start-up date of each plant (1917 to 1946) to 1990.
For the job analysis, 15,465 crude department names and 47,693 crude job titles were grouped into 1668 unique department and job pairs (UDJobs), which represented a job title linked to a specific department within each plant. Every UDJob was evaluated according to a set of job elements related to airborne fiber exposure.
The distribution of the cohort person-years by UDJob and the job-exposure elements was then evaluated. The results show the main departments and jobs that employed the workers for each plant. The distribution of person-years varies across the job-exposure elements.
The same job title was used in different departments within and across plants. When job titles not linked to departments were evaluated, the values of the job-exposure elements varied considerably across all plants and within plant.
In conclusion:
(1) exposure misclassification could occur if job title alone were used for the exposure assessment;
(2) the job-exposure elements analysis provides an efficient way to identify major job determinants of exposure without relying on the more detailed, resource-intensive task-based approach; and (
3) the evaluation of the cohort person-years by UDJobs and job-exposure elements is an effective way to identify which plants, departments, and jobs have sufficient information for making precise risk estimates in the broader epidemiologic study. - Shipyard industry, see CFR 29 1915 https://www.osha.gov/pls/oshaweb/owastand.display_standard_group?p_toc_level=1&p_part_number=1915
and also this document on air contaminants https://www.osha.gov/pls/oshaweb/owadisp.show_document?p_table=STANDARDS&p_id=10286 - Stayner, Leslie T., DavidA Dankovic, and RichardA Lemen. "Occupational exposure to chrysotile asbestos and cancer risk: a review of the amphibole hypothesis." American Journal of Public Health 86, no. 2 (1996): 179-186.
- U.S. EPA, OVERVIEW OF PARTICLE AIR POLLUTION (PM2.5 AND PM10) AIR QUALITY COMMUNICATION WORKSHOP [PDF of a power point presentation],
San Salvador, El Salvador
April 16-17, 2012 retrieved 2018/07/11, original source: https://www.epa.gov/sites/production/files/2014-05/documents/huff-particle.pdf
Note: this presentation does not specifically focus on fiberglass. Excerpts:
Particulate matter (PM) is a general term for very small solid and liquid particles in the atmosphere
There are many different sources of PM, including natural and anthropogenic (man-made) sources
PM is hazardous to human health – it causes acute and chronic effects to the respiratory and cardiovascular systems
PM causes a variety of human health and economic impacts each year (e.g., mortality, morbidity, DALYs, lost income from work absences, costs of health care) - Williams, Malcolm, and Peter Roger McClure. "TOXICOLOGICAL PROFILE FOR SYNTHETIC VITREOUS FIBERS." [PDF] (2004) U.S. CDC, U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Public Health Service
Agency for Toxic Substances and Disease Registry
Excerpts from the document's
PUBLIC HEALTH STATEMENT :
A fiber is simply a long, slender particle. Technically, to be counted as a fiber, the particle must be at least 5 micrometers long (1 micrometer equals 1/1,000,000 of a meter and has the symbol μm), and have an aspect ratio of at least 3 to 1 or sometimes 5 to 1 (the aspect ratio is the ratio of a fiber’s length to its diameter).
The diameter of a fiber is an important property because very thin fibers are more easily suspended in air than thick fibers, and they can be breathed in and deposited deep in the lungs.
Only very thin fibers with diameters less than 3 μm are able to be breathed into the lower respiratory tract of humans. Thicker fibers are deposited on the mucous-lined surface of the upper respiratory tract, which includes the nose and mouth.
The World Health Organization (WHO) counts respirable fibers as particles with lengths greater than 5 μm, diameters less than 3 μm, and aspect ratios ≥3:1. Depending upon the way that they are produced, fibers can have relatively large or small diameters. Generally speaking, glass wool, rock wool, slag wool, and refractory ceramic fibers have the smallest diameters, while continuous filament glass fibers have the largest diameters. - op. cit. p. 2
Synthetic vitreous fibers do not evaporate into air or dissolve in water. - Op. cit. p.3.
In 2002, the International Agency for Research on Cancer (IARC) considered all of the evidence regarding the possible carcinogenicity of synthetic vitreous fibers. Much of the evidence was collected in the 1990s and was not available for earlier assessments made by the U.S. Department of Health and Human Services (DHHS). IARC determined that refractory ceramic fibers are possibly carcinogenic to humans because of their high biopersistence.
IARC also determined that insulation glass wool, stone wool, and slag wool, and continuous filament glass were not classifiable as to carcinogenicity to humans because of inadequate evidence of carcinogenicity in humans and the relatively low biopersistence of these materials.
EPA has not assessed the potential carcinogenicity of glass wool, stone wool, slag wool, or continuous filament glass, but has classified refractory ceramic fibers as a probable human carcinogen. - Op. Cit. p. 7
Health Protection Recommendation:
In 1999, a Health and Safety Partnership Program was established as a voluntary workplace safety program for workers involved in the manufacture, fabrication, installation, and removal of glass wool, rock wool, and slag wool products. The program was established as a result of negotiations between the OSHA, the North American Insulation Manufacturers Association, the National Insulation Association, and the Insulation Contractors Association of America.
The program established a voluntary 8-hour time-weighted average (TWA) permissible exposure limit (PEL) of 1 respirable fiber per cc of air.
Under this agreement, respirable fibers are counted as particles with length greater than 5 μm, diameter less than 3 μm, and aspect ratio greater than or equal to 3:1. The agreement specifies that when the PEL is exceeded in a workplace (such as when insulation is blown into attics or removed), workers will wear NIOSH certified dust respirators. - Op. Cit. p. 11 - Wilson, James, Virginia Murray, and J. Nick Kettle. "The July 2005 London bombings: environmental monitoring, health risk assessment and lessons identified for major incident response." (2009): 642-643.
- [5] World Health Organization International Agency for Research on Cancer - IARC Monographs on the Evaluation of Carcinogenic Risks to Humans - VOL 81 Man-Made Vitreous Fibers, 2002, IARCPress, Lyon France, pi-ii-cover-isbn.qxd 06/12/02 14:15 Page i - World Health Organization, 1/21/1998.
-Fiberglass insulation is an example of what IARC refers to as man made vitreous fiber - inorganic fibers made primarily from glass, rock, minerals, slag, and processed inorganic oxides.
This article provides enormous detail about fiberglass and other vitreous fibers, and includes fiberglass exposure data. - Yang, Li-Jun, Xiao-fang WANG, and Ze-Liang BAO. "Occupational Hygiene of Production Line in Fiberglass Company." Chinese Journal of Public Health Engineering 10, no. 3 (2011).
Excerpt:
Occupational Hygiene of Production Line in Fiberglass Company. - Youk, Ada O., Gary M. Marsh, Roslyn A. Stone, Jeanine M. Buchanich, and Thomas J. Smith. "Historical cohort study of US man-made vitreous fiber production workers: III. Analysis of exposure-weighted measures of respirable fibers and formaldehyde in the nested case-control study of respiratory system cancer." Journal of occupational and environmental medicine 43, no. 9 (2001): 767-778.
Abstract:
The most recent findings of our nested case-control study of respiratory system cancer (RSC) among male fiberglass workers showed some evidence of elevated RSC risk associated with non-baseline levels of average intensity of exposure (AIE) to respirable fibers (RFib).
When adjusted for smoking, this was not statistically significant, and no trend was apparent with increasing levels of exposure.
Similar findings for RSC were noted for both cumulative exposure (Cum) and AIE to formaldehyde (FOR). In this reanalysis of our nested case-control study, we explored a possible exposure–response relationship between RSC and exposure to RFib or FOR using exposure weighting as an alternative characterization of exposure.
Because of the uncertainties in selecting an appropriate exposure-weighting scheme, a range of plausible time lags and unlagged/lagged time windows was considered. As in the initial analysis of the nested case-control study, RFib and FOR exposures were categorized at the deciles of the RSC case distribution.
For none of the exposure weighting schemes considered did we observe an increasing RSC risk with increasing levels of RFib_Cum or RFib_AIE.
The exposure-weighted estimated risk ratios (RR) for both RFib_Cum and RFib_AIE were generally lower than those obtained from an unweighted model. For FOR_Cum, RRs were generally lower for the time-lagged and unlagged time window models than for the unweighted models, although some decile-specific RRs were higher for the lagged time window models.
The exposure-weighted RRs for FOR_AIE were generally lower than the unweighted RRs for all of the weighting schemes considered. This reanalysis in terms of categorized exposures reveals no exposure–response relationships that were undetected in the original analysis where unweighted exposure measures were used. In the schemes considered, exposure weighting generally reduced the estimated risk of RSC. - Zhang, Yunlin, Bing Zhang, Xin Wang, Junsheng Li, Sheng Feng, Qiaohua Zhao, Mingliang Liu, and Boqiang Qin. "A study of absorption characteristics of chromophoric dissolved organic matter and particles in Lake Taihu, China." Hydrobiologia 592, no. 1 (2007): 105-120.
Note: this is NOT a fiberglass particle study but reports on absorption of very small particles by non-phytoplankton particles and phytoplankton.
Canadian & Other Fiberglass Hazard Resources - Yacht-Makers Lung research
In Canada see http://www.canoshweb.org/ Canada's National Workplace Health & Safety Website
There you'll see a provincial map that gives contact information by province.
Canadians are less fearful of fiberglass than some Yanks. The Health Canada discussion of workplace IAQ mentions mold and general hazards and housekeeping
see
- Canadian Centre for Occupational Health and Safety CCOHS: Indoor Air Quality - www.ccohs.ca/topics/hazards/workplace/iaq/
- "Fiberglass and School Health", Not a Health Canada official site, but this other Canadian health source discusses fiberglass hazards in schools.
casle.ca/fibreglass-insulation-and-school-health-2/ - Here is a U.S. MIT MSDS on fiberglass
http://web.mit.edu/rocketteam/www/usli/MSDS/Fiberglass%20(differnt%20supplier).pdf - CCOHS FAQs on IAQ includes this comment on Canadian laws or guidelines for IAQ - not specific to fiberglass
Many Canadian jurisdictions do not have specific legislation that deals with indoor air quality issues. In the absence of such legislation, the "general duty clause" applies. This clause, common to all Canadian occupational health and safety legislation, states that an employer must provide a safe and healthy workplace. Thus, making sure the air is of good quality is the employer's duty.
Several organizations* have published recommended guidelines for indoor air quality. For example, Health Canada has prepared a number of publications on air quality. In the United States, the Occupational Safety and Health Administration (OSHA) has compiled information on Indoor Air Quality.
In addition, IAQ is implied in most building codes as design and operation criteria. Building codes in Canada and the U.S. generally refer to the American Society of Heating, Refrigerating, and Air Conditioning Engineers* (ASHRAE) Standard 62.1-2010 - Ventilation for Acceptable Indoor Air Quality (or previous versions), or other acceptable standards.
It is important to understand that most IAQ standards and guidelines are established to ensure the comfort of workers. So these values tend to be lower than regulatory values that are set to protect workers from possible health based hazards.
*We have mentioned these organizations as a means of providing a potentially useful referral.
You should contact these organizations directly for more information. < - "OSH Answers Fact Sheets, Indoor Air Quality - General, Are there laws or guidelines for IAQ [in Canada]?", retrieved 2016/02/16, original source: http://www.ccohs.ca/oshanswers/chemicals/iaq_intro.html
Fiberglass hazards in boatbuilding
An industry where fiberglass hazards have long been discussed as "Yachtmaker's Lung Disease" . You'll see that styrene exposure hazards are also discussed.
- Brigham, Christopher R., and Philip J. Landrigan. "Safety and health in boatbuilding and repair." American journal of industrial medicine 8, no. 3 (1985): 169-182.
- Deichmann, William B. "Potential Health Hazards of Materials Used in Boating." JAMA 213, no. 5 (1970): 759-764.
- Kaufman, Joel D., Martin A. Cohen, Susan R. Sama, Joanne W. Shields, and John Kalat. "Occupational skin diseases in Washington State, 1989 through 1993: using workers' compensation data to identify cutaneous hazards." American journal of public health 88, no. 7 (1998): 1047-1051.
- Ruttenberg, David, Evan Dryson, Chris Walls, and Nicky Curran. "Hazards associated with the boat building industry in New Zealand: an OSH audit." New Zealand medical journal 114, no. 1132 (2001): 225.
- Sullivan, Brian J. "Styrene exposure in a fiberglass boat manufacturing operation." Applied occupational and environmental hygiene 18, no. 7 (2003): 496-498.
- Volkman, Kristen K., James G. Merrick, and Michael C. Zacharisen. "Yacht-maker's lung: A case of hypersensitivity pneumonitis in yacht manufacturing." Wisconsin Medical Journal 105, no. 7 (2006): 47-50.
- Wareham-Fowler, Stacey, and Ken Fowler. "Risk Perception, Safety Behaviour, Employment Precarity and Community Attachment: The Case of Newfoundland and Labrador Fibreglass Boatbuilding Workers." Policy and Practice in Health and Safety 8, no. 1 (2010): 43-60.
...
...
Continue reading at FIBERGLASS HAZARDS - home or select a topic from the closely-related articles below, or see the complete ARTICLE INDEX.
Or see these
Recommended Articles
- FIBERGLASS HAZARDS - home
- AIR FILTERS, FIBERGLASS PARTICLES
- DUST ANALYSIS for FIBERGLASS
- FIBERGLASS ASBESTOS COMBINATIONS
- FIBERGLASS DETECTION in BUILDING AIR & DUST
- FIBERGLASS ENVIRO-SCARE
- FIBERGLASS FRAGMENT HAZARDS in AIR or DUST
- FIBERGLASS HAZARD RESEARCH
- FIBERGLASS INSULATION EXPOSURE LIMITS
- FIBERGLASS PARTICLE CONTAMINATION TEST
- FIBERGLASS REINFORCED PLASTICS
- FIBERGLASS SHEDDING from MATTRESSES
- FORMALDEHYDE in FIBERGLASS INSULATION
- FIBERGLASS HVAC DUCTS
- FIBERGLASS IDENTIFICATION in the LAB
- FIBERGLASS INSULATION EXPOSURE LIMITS
- FIBERGLASS INSULATION IDENTIFICATION & PROPERTIES
- FIBERGLASS INSULATION MOLD
- FORMALDEHYDE GAS SOURCES & HAZARDS RESEARCH
- MINERAL WOOL - ROCK WOOL INSULATION
- MORGELLONS SYNDROME
- TEST PROCEDURE for MOLD in FIBERGLASS
Suggested citation for this web page
FIBERGLASS HAZARD RESEARCH at InspectApedia.com - online encyclopedia of building & environmental inspection, testing, diagnosis, repair, & problem prevention advice.
Or see this
INDEX to RELATED ARTICLES: ARTICLE INDEX to FIBERGLASS HAZARDS
Or use the SEARCH BOX found below to Ask a Question or Search InspectApedia
Ask a Question or Search InspectApedia
Share this article:Try the search box just below, or if you prefer, post a question or comment in the Comments box below and we will respond promptly.
Search the InspectApedia website
Note: appearance of your Comment below may be delayed: if your comment contains an image, photograph, web link, or text that looks to the software as if it might be a web link, your posting will appear after it has been approved by a moderator. Apologies for the delay.
Only one image can be added per comment but you can post as many comments, and therefore images, as you like.
You will not receive a notification when a response to your question has been posted.
Please bookmark this page to make it easy for you to check back for our response.
IF above you see "Comment Form is loading comments..." then COMMENT BOX - countable.ca / bawkbox.com IS NOT WORKING.
In any case you are welcome to send an email directly to us at InspectApedia.com at editor@inspectApedia.com
We'll reply to you directly. Please help us help you by noting, in your email, the URL of the InspectApedia page where you wanted to comment.
Citations & References
In addition to any citations in the article above, a full list is available on request.
- In addition to citations & references found in this article, see the research citations given at the end of the related articles found at our suggested
CONTINUE READING or RECOMMENDED ARTICLES.
- Carson, Dunlop & Associates Ltd., 120 Carlton Street Suite 407, Toronto ON M5A 4K2. Tel: (416) 964-9415 1-800-268-7070 Email: info@carsondunlop.com. Alan Carson is a past president of ASHI, the American Society of Home Inspectors.
Thanks to Alan Carson and Bob Dunlop, for permission for InspectAPedia to use text excerpts from The HOME REFERENCE BOOK - the Encyclopedia of Homes and to use illustrations from The ILLUSTRATED HOME .
Carson Dunlop Associates provides extensive home inspection education and report writing material. In gratitude we provide links to tsome Carson Dunlop Associates products and services.
 |
HOME | ABOUT | ASK a QUESTION | CONTACT | CONTENT USE POLICY | DESCRIPTION | POLICIES | PRIVACY | |
| © 2026 - 1985 Publisher InspectApedia.com - Daniel Friedman | |||||||||